
PARTIAL KNEE REPLACEMENT
What is the Patella?
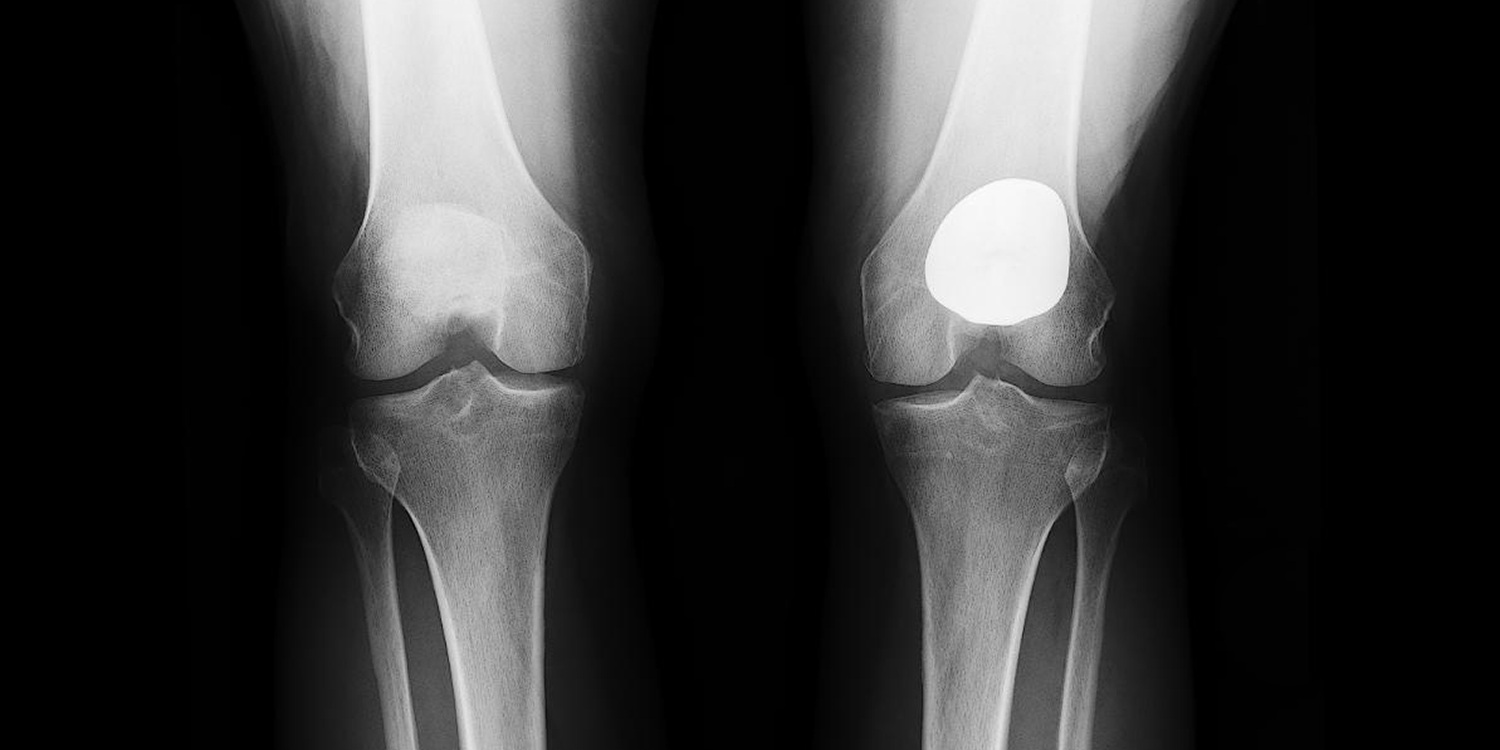
A Patella is: The kneecap, or a thick, triangular bone which articulates with the femur (thigh bone) and covers and protects the front surface of the knee joint.
What are the Symptoms Indicating the Need for Knee Replacement Surgery?
Symptoms indicating the need for a replacement surgery:
- Isolated knee pain
- Arthritis in the front of the knee
- Pain when climbing stairs or walking up an incline
Underlying causes for knee replacement surgery include:
- History of patella instability or dislocations
- A severe injury to the patella (kneecap), such as a fracture
- Malalignment, in which there is an increased load on the patella and early cartilage wear
- Osteoarthritis without a specific origin
- Rheumatoid arthritis
- Post-traumatic arthritis
Surgical Treatment
Am I a candidate for a partial knee replacement?
You are a candidate for a partial knee replacement if you have severe knee pain and examination findings that point towards arthritis of the knee. Additionally, you have tried non-surgical treatments, such as injections and physical therapy, with no relief of symptoms. This surgery is indicated when there is damage to the cartilage in only one compartment of the knee. This is evaluated through the use of MRI and XRAY. Cartilage is the shiny, smooth coating at the end of bones. It protects the bone and allows the bones to move smoothly and efficiently. There are 3 compartments of the knee: medial tibial-femoral (inside part of the knee), lateral tibial-femoral (outside part of the knee), and patellar-femoral (behind the kneecap).
What caused my knee to become arthritic in this compartment?
Knees can become arthritic for a variety of reasons. Because they bear significant stress over the course of our life, some degeneration is simply the result of wear and tear. This can also be due to trauma to the knee, malalignment of the knee, or genetic predisposition.
What happens during a partial knee replacement surgery?
A vertical incision, is made in the front of the knee. Focusing on the compartment being replaced, the damaged bone and cartilage in the knee joint are removed and the worn ends of the bone are shaped to fit the implant, which is inserted and attached to the bones with cement. The exact type of implants used is called Zimmer for the patellofemoral replacement. The implants are made of cobalt chrome and high molecular weight plastic. The incision is then closed with absorbable sutures and Dermabond, a surgical glue and tape. Unlike the total knee replacement (TKR), you will keep your ACL (anterior cruciate ligament), PCL (posterior cruciate ligament), and other compartments of your knee.
How long will my implants last?
The lifetime of the implants varies, depending on the patient’s lifestyle and compliance with post-operative instructions, the fit of the implants, and, of course, chance. However, 90% of patients have functional implants 15 years after their partial knee replacement surgery. The reasons for failure include infection, implant instability, conversion to TKR, or fracture.
How long will I stay in the hospital?
This surgery is can be in-patient procedure, meaning one night stay in the hospital after surgery, or it can be done as ambulatory surgery, meaning you go home the same day of surgery. This is in part determined by your age, health status, and your post-op recovery.
What are the possible risks and complications of surgery?
As with any surgery there is a risk of DVT, nerve damage, and postoperative infection. Specific risks and complications include but aren’t limited to infection, fracture, post-op stiffness, hardware complications, and conversion to TKR if arthritis develops in the other compartments of the knee.
When can I drive? When can I go back to work?
You may not drive while taking the pain medication. Most patients can drive after 3-4 weeks, but it is very important that you make sure you have full control of your injured leg prior to returning to driving. The recovery time needed before returning to work varies depending on your type of work, but is at least 3 weeks for office work and 8 weeks for manual labor.
Can I return to jogging, skiing, and other high-impact or contact sports?
If you comply with your physical therapy and post-operative instructions, achieving total muscle recovery, then there are no restrictions on any type of activity. However, studies have shown that, because the implants are mechanical devices, high loads cause them to wear out more quickly, resulting in a higher risk of needing a revision. You should avoid running activities. Please see Your Surgery and Physical Therapy for more information on this condition.
Am I a candidate for PFJR + MPFL?
You are a candidate if you have patellar instability (kneecap dislocation) and front knee pain with examination findings that point towards kneecap arthritis (patellofemoral osteoarthritis). This is evaluated through the use of MRI and XRAY.
What is osteoarthritis and how does it occur?
Cartilage is the shiny, smooth coating at the end of bones. It protects the bone and allows the bones to move smoothly and efficiently. When this cartilage thins or becomes damaged, it’s called osteoarthritis. It can be caused by a number of factors including genetics and injury.
What is the medial patellofemoral ligament (MPFL) and how is it damaged?
The MPFL is a ligament that stabilizes the patella (kneecap) and keeps it from displacing laterally. It is disrupted when someone dislocates his/her patella. When the kneecap dislocates towards the outside, this stretches the ligament on the inside of the knee, which is trying to keep the kneecap in place. This can result in either a tear of the MPFL or a detachment of the ligament from the bone. Additionally, when the kneecap goes out of place, and then back in, it knocks on the lateral femoral condyle (part of the thigh bone), which can often result in an injury to the cartilage and contribute to arthritis.
What does the surgery entail?
A vertical incision is made in the front of the knee. Focusing on the patellofemoral compartment, the damaged bone and cartilage in the knee joint are removed and the worn ends of the bone are shaped to fit the implant, which is inserted and attached to the bones with cement. The exact type of implants used is called Zimmer. The implants are made of cobalt chrome and high molecular weight plastic. Then, the injured MPFL ligament will be replaced with a graft, usually a quadriceps tendon from the same leg or a cadaver allograft. The graft is attached to the femur via small absorbable screws that hold the graft in place and an attach to the femur. The incision is then closed with absorbable sutures and Dermabond, a surgical glue and tape.
How long will I stay in the hospital?
This surgery is an in-patient procedure, meaning you will stay in the hospital after surgery. You will then be discharged home. Hospital stay is usually a one night stay.
What are the possible risks and complications of surgery?
As with any surgery there is a risk of DVT, nerve damage, and postoperative infection. Specific risks and complications include but aren’t limited to re-tear, infection, fracture, post-op stiffness, hardware complications, and possible conversion to TKR if arthritis develops in the other compartments of the knee in the future.
When can I drive? When can I go back to work?
You may not drive while taking pain medication. In addition, if it is your right knee that had surgery, you will not be able to drive for approximately 6 weeks after surgery or until the brace is removed. The recovery time needed before returning to work varies depending on your type of work, but is at least 3 weeks for office work and 8 weeks for manual labor.
Can I return to jogging, skiing, and other high-impact or contact sports?
If you comply with your physical therapy and post-operative instructions, achieving total muscle recovery, then there are no restrictions on any type of activity. However, studies have shown that, because the implants are mechanical devices, high loads cause them to wear out more quickly, resulting in a higher risk of needing a revision. You should avoid running activities. Please see Your Surgery and Physical Therapy for more information on this condition.